Books of Interest
Website: chetyarbrough.blog
Rethinking Medications (Truth, Power, and the Drugs You Take)
By: Jerry Avorn
Narrated By: Jerry Avorn MD

Jerry Avorn (Author, professor of medicine at Harvard Medical School where he received his MD, Chief Emeritus of the Division of Pharmacoepidemiology and Pharmacoeconomics)
Doctor Avorn enlightens listener/readers about drug industry’ costs, profits, and regulation. Avorn explains how money corrupts the industry and the FDA while encouraging discovery of effective drug treatments. The cost, profits, and benefits of the industry revolve around research, discovery, medical efficacy, human health, ethics, and regulation.
Drug manufacture is big business.

Treatments for human maladies began in the dark ages when little was known about the causes of disease and mental dysfunction. Cures ranged from spirit dances to herbal concoctions that allegedly expelled evil, cured or killed its followers and users. The FDA (Food and Drug Administration) did not come into existence until 1930, but its beginnings harken back to the 1906 Pure Food and Drug Act signed into law by Theodore Roosevelt. The FDA took on the role of reviewing scientific drug studies for drug treatments that could aid health recovery for the public. The importance of review was proven critical by incidents like that in 1937, when 107 people died from a Sulfanilamide drug which was found to be poisonous. From that 1937 event forward, the FDA required drug manufacturers to prove safety of a drug before selling it to the public. The FDA began inspecting drug factories while demanding drug ingredient labeling. However, Avorn illustrates how the FDA was seduced by Big Pharma’ to offer drug approvals based on flawed or undisclosed research reports.

Dr. Martin Makary (Dr. Makary was confirmed as the new head of the FDA on March 25, 2025. He is the 27th head of the Department. He is a British-American surgeon and professor.)
What Dr. Avorn reveals is how the FDA has either failed the public or been seduced by drug manufacturers to approve drugs that have not cured patients but have, in some cases, harmed or killed patients. It will be interesting to see what Dr. Marin Makary can do to improve FDA’s regulation of drugs. Avorn touches on court cases that have resulted in huge financial settlements by drug manufacturing companies and their stockholders. However, he notes the actual compensation received by individually harmed patients or families is miniscule in respect to the size of the fines; not to mention many billions of dollars the drug companies received before unethical practices were exposed. Avorn notes many FDA’ research and regulation incompetencies allowed drug companies to hoodwink the public about drug companies’ discovered but unrevealed drug side-effects.
A few examples can be easily found in an internet search:
1) Vioxx (Rofecoxib), a pain killer, had to be withdrawn from use in 2004 because it was linked to increased risk of heart attacks and strokes. It was removed from the market in 2004.
2) Fen-Phen (Fenfluramine/Phentermine), a weight-loss drug had to be taken off the market in 1997 because of severe heart and lung complications.
3) Accutane was used to cure acne but was found to be linked to birth defects and had to be withdrawn in 2009.
4) Thalidomide was found to cause birth defects to become repurposed for treatment of certain cancers.
5) A more recent failure of the FDA is their failure to regulate opioids like OxyContin that resulted in huge fines to manufacturers and distributors of the drug.
Lobbyists are hired by drug companies to influence politicians to gain support of drug companies. In aggregate, this chart shows the highest-spending lobbyists in the 3rd Qtr. of 2020 were in the medical industry.

Dr. Avorn argues Big Pharma’s lobbying power has unduly influenced FDA to approve drugs that are not effective in treating patients for their diagnosed conditions. Avorn infers Big Pharma is more focused on increasing revenue than effectively reviewing drug manufacturer’ supplied studies. Avorn argues the FDA has become too dependent on industry fees that are paid by drug manufacturers asking for expedited drug approvals. Avorn infers the FDA fails to demand more documentation from drug manufacturers on their drug’ research. The author suggests many approved opioids, cancer treatment drugs, and psychedelics have questionable effectiveness or have safety concerns. Misleading or incomplete information is provided by drug companies that makes applications an approval process, not a fully relevant or studied action on the efficacy of new drugs.

Avorn is disappointed in the Trump administrations’ selection of Robert Kennedy as the U.S. Secretary of Health and Human Services because of his lack of qualification.
The unscientific bias of Kennedy and Trump in regard to vaccine effectiveness reinforces the likelihood of increased drug manufacturers’ fees that are just a revenue source for the FDA. Trump will likely reward Kennedy for decreasing the Departments’ overhead by firing research scientists and increasing the revenues they collect from drug manufacturers seeking drug approvals.
Trump sees and uses money as the only measure of value in the world.

It is interesting to note that Avorn is a Harvard professor, a member of one of the most prestigious universities in the world. Harvard is being denied government grants by the Trump administration, allegedly because of Harvard’s DEI policy. One is inclined to believe diversity, equity, and inclusion are ignored by Trump because he is part of the white ruling class in America. Trump chooses to stop American aid to the world to reduce the cost of government. American government’s decisions to starve the world and discriminate against non-whites is a return to the past that will have future consequences for America.
Next, Avorn writes about the high cost of drugs, particularly in the United States. Discoveries are patented in the United States to incentivize innovation, but drug companies are gaming that Constitutional right by slightly modifying drug manufacture when their patent rights are nearing expiration. They renew their patent and control the price of the slightly modified drug that has the same curative qualities. As publicly held corporations, they are obligated to keep prices as high as the market allows. The consequence leaves many families at the mercy of their treatable diseases because they cannot afford the drugs that can help them.
Martin Shkreli, American investor who rose to fame and infamy for using hedge funds to buy drug patents and artificially raise their prices to only increase revenues.

The free market system in America allows an investor to buy a drug patent and arbitrarily raise its price. Avorn suggests this is a correctable problem with fair regulation and a balance between government sponsored funding for drug research in return for public funding. Of course, there are some scientists like Jonas Salk in 1953 who refused to privately patent the polio vaccine because it had such great benefit to the health of the world.

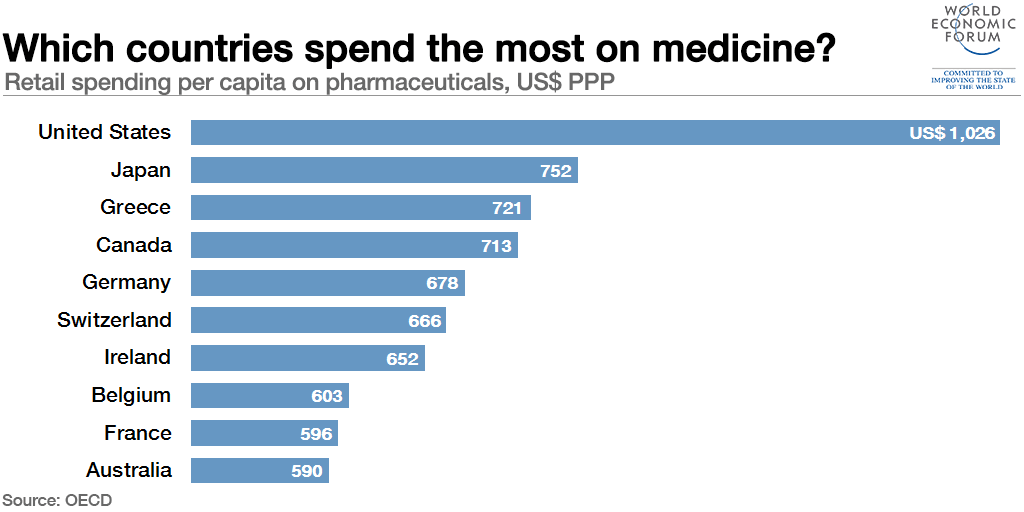
Avorn notes the 1990’s drug costs in the U.S. are out of control.
Only the rich are able to pay for newer drugs that cost hundreds of thousands of dollars per year. Americans spend over $13,000 per year per person while Europe is around $5,000 and low-income countries under $500 per year. These expenditures are to extend life which one would think make Americans live longest. Interestingly, America is not even in the top 10. Hong Kong’s average life expectancy is 85.77 years, Japan 85. South Korea 84.53. The U.S. average life expectancy is 79.4. To a cynic like me, one might say what’s 5 or 6 more years of life really worth? On the other hand, billionaires and millionaires like Peter Thiel and Bryan Johnson have invested millions into anti-aging research.
Avorn reinforces the substance of Michael Pollan’s book “How to Change Your Mind” which reenvisions the value of hallucinogens in this century.
Avorn notes hallucinogens efficacy is reborn in the 21st century to a level of medical and social acceptance. Avorn is a trained physician as opposed to Pollan who is a graduate with an M.A. in English, not with degrees in science or medicine.

In reviewing Avorn’s informative history, it is apparent that patients should be asking their doctors more questions about the drugs they are taking.
Drugs have side effects that can conflict with other drugs being taken. In this age of modern medicine, there are many drugs that can be effective, but they can also be deadly. Drug manufacturers looking at drug creation as only revenue producers is a bad choice for society.
Avorn’s history of the drug industry shows failure in American medicines is more than the mistake of placing an incompetent in charge of the U.S.

Taking money away from research facilities diminishes American innovation in medicine and other important sciences. However, research is only as good as the accuracy of its proof of efficacy for the treatment of disease and the Hippocratic Oath of “First, do no harm”. A government designed to use public funds to pick winners and losers in the drug industry threatens human health. Only with the truth of science discoveries and honest reporting of drug efficacy can a physician offer hope for human recovery from curable diseases.