
Audio-book Review
By Chet Yarbrough
(Blog:awalkingdelight)
Website: chetyarbrough.blog
Do No Harm: Stories of Life, Death, and Brain Surgery
Written by: Henry Marsh
Narration by: Jim Barclay

HENRY MARSH (BRITISH NEUROSURGEON AND AUTHOR)
An interesting insight offered by Henry Marsh’s memoir, “Do No Harm”, is a contrast between American and British Medicine. Marsh’s candor about his life and profession surprise his audience and endear his curmudgeonly personality. The surprise is in Marsh’s profound empathy and personal conflicts over neurosurgical decisions.
Marsh’s endearment comes from explicit “f-word” rants about incompetence, technology, and bureaucracy. In addition to his rants, Marsh endears himself to an audience by explaining the distinction between a physician’s self-confidence and hubris. Marsh suggests physicians need understanding and competence; not undue preciousness, and pride-full medical knowledge. Jim Barclay’s narration perfectly suits the tone of Marsh’s memoir.

Marsh is able to enter into medicine with little pre-medical education in the sciences.
Either by dint of a formidable intellect or a quirk of the British education system (maybe both), Marsh takes all his science courses after deciding to become a doctor. One doubts an American medical school would have considered his application in the 1960 s.
Marsh graduates and begins his career in medicine under the guidance of experienced physicians. As he acquires experience, he chooses to specialize in neurosurgical medicine under the supervision of a Consulting Neurological Physician. The Consultant (a neurology physician trainee’s guide) works within the English national health care system as a qualified physician who supervises aspiring neurological physicians. This consultant chooses cases for trainees; under varying levels of supervision.
Though a neurological procedure may be done by a trainee, the consulting physician is responsible. This appears to be similar to internships in the United States. However, an interesting difference is in the insurance for interns.

MEDICAL INTERNSHIPS- English hospitals carry a trust to protect physicians from mistakes made in treating patients.
The UK’s physician-group self-insurance may be a distinction without a difference but, as in all medical insurance systems, mistakes do occur, and patients are harmed. The difference between physician-group self-insurance and American physician’ private insurance raises the specter of limited settlement for egregious mistakes. On the other hand, it suggests British physicians are more likely to be more forthcoming on mistakes that are made.
Marsh completes his trainee experience and decides to become a Consulting Neurological Physician in the national health care system. Marsh interestingly reveals several mistakes he and his trainees make during his years of consultancy. In revealing those mistakes, a listener pauses to think about risks of patients who depend on English’ or American’ medical services. Marsh’s stories of mistakes reflect on medical training, family apologies, and personal anguish over patient’ quality-of-life and death issues.

Marsh explains, at best a Consultant Surgeon expects to learn from surgical mistakes to avoid repetition.
The worst, for Marsh, is the apologies to families for the mistakes that are made. In contrast to Marsh’s way of addressing mistakes, American physicians seem more likely to avoid family apologies; while hiding behind legal and insurance company shields.

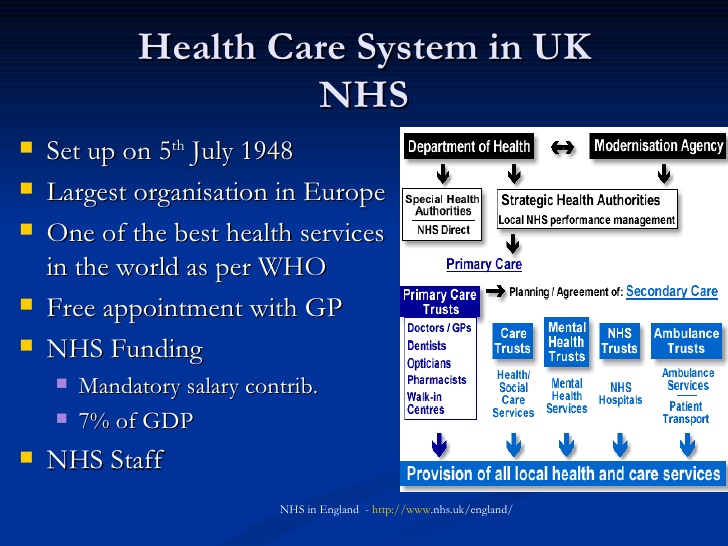
A more subtle message in Marsh’s book is the failure of the English National Health Service to provide adequate care for the general population; e.g. its long lines of patients who wait for attention when rapidly growing tumors are destroying a patient’s neurological system.
Doctor/patient ratios in 2016 were 2.6/1,000 people in America. In 2018, the doctor/patient ratio was 2.8/1,000 in the United Kingdom. This raises the question of how long would Americans have to wait in line with a national health care system? Some argue physician assistants could be trained to take care of less serious medical issues. That would spread the burden of patient treatment.
Marsh complains of inadequate bed availability for patients that need operations. Financing for the National Health Service is inadequate for the number of patients that need help. This seems a likely consequence of an American national health care system.
Marsh notes that he carries private health insurance to supplement his family’s medical needs. At the same time, he infers private hospital services tend to gouge patients for their medical service; in part, from charges for unnecessary tests and superfluous operations.
Marsh attacks the bureaucratic nature of the National Health Service that hires hospital administrators who are directed to reduce costs; regardless of patient’ load or patient’ need. Technological improvements for England’s National Health Service are delayed because of lack of financing, poor administration, and inadequate training. These are maladies that will plague a national health care system in the United States.
Marsh leavens his criticism of England’s national health care by writing of his experience in the former U.S.S.R. (specifically Ukraine) where problems are monumentally greater.
In the end, America’s effort to improve national health care is tallied in one’s mind against the current English picture painted by Marsh. For medical patients, the English system seems riskier than the American system. Doctors in England seem more insulated from medical mistakes. If doctors are more insulated, they may take more risks; i.e. risks that can lead to patient’ disablement or death. The American system, if one can afford the service, seems more conservative and less likely to take risks.
It seems England’s national health care offers a level of societal comfort because there is hope for affordable treatment. On the other hand, Marsh clearly shows how government bollixes National Health Care with inadequate funding and a bumbling administrative system. Some would say this is why the U. S. should not nationalize health care.
Marsh notes England’s private system has not met the needs of citizens who can afford additional service. The private system suffers from human nature’s folly; i.e. the lure of wealth at the expense of fairly priced or truly needed medical treatment.

Marsh suggests the private system suffers from human nature’s folly; i.e. the lure of wealth at the expense of fairly priced or truly needed medical treatment.
Is medical health service a human right or privilege? One draws their own conclusion about British and American Medicine. Marsh shows the monumental problems of affordable health care in England.
A listener of “Do No Harm” infers problems of the British system for medical care will challenge America’s desire for universal health care. Dr. Marsh’s answer seems to revolve around empathy for all human beings; i.e. regardless of whether a country has a nationalized or private health care system.
